
More Information
Submitted: March 15, 2021 | Approved: March 17, 2021 | Published: March 18, 2021
How to cite this article: Chen YH, Wang SS, Hu SY. Ketamine-related uropathy and cholangiopathy. J Clin Med Exp Images. 2021; 5: 002-002.
DOI: 10.29328/journal.jcmei.1001018
Copyright License: © 2021 Chen YH, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.

Ketamine-related uropathy and cholangiopathy
Yi-Hsuan Chen1, Shian-Shiang Wang2 and Sung-Yuan Hu1,3-5*
1Department of Emergency Medicine, Taichung Veterans General Hospital, Taiwan
2Division of Urology, Department of Surgery, Taichung Veterans General Hospital, Taiwan
3School of Medicine, Chung Shan Medical University, Taiwan
4Institute of Medicine, Chung Shan Medical University, Taiwan
5Department of Nursing, College of Health, National Taichung University of Science and Technology, Taichung, Taiwan
*Address for Correspondence: Sung-Yuan Hu, Department of Emergency Medicine, Taichung Veterans General Hospital, 1650 Taiwan Boulevard Sect. 4, Taichung 40705, Taiwan, Tel: +886 4 23592525; ext 3601; Fax: +886 4 23594065; Email: [email protected]
A 23-year-old man had a 2-year history of ketamine abuse and presented intermittent abdominal pain, urinary urgency and dysuria for one year. Two weeks ago, laboratory analysis showed within normal limits. This time, he visited our emergency department due to hematuria and bilateral flank pain. CT scan and MRI revealed bilateral hydronephrosis, hydroureter, irregular thickened wall of urinary bladder, and fusiform common bile duct with distal stenosis (Figure 1A, 1B, 1C). Cystoscopy demonstrated ketamine-associated ulcerative cystitis (KAUC) (Figure 1D). Condition became better after bilateral percutaneous nephrostomy and ceasing ketamine abuse. Figure 2 showed serial renal and liver function profiles.
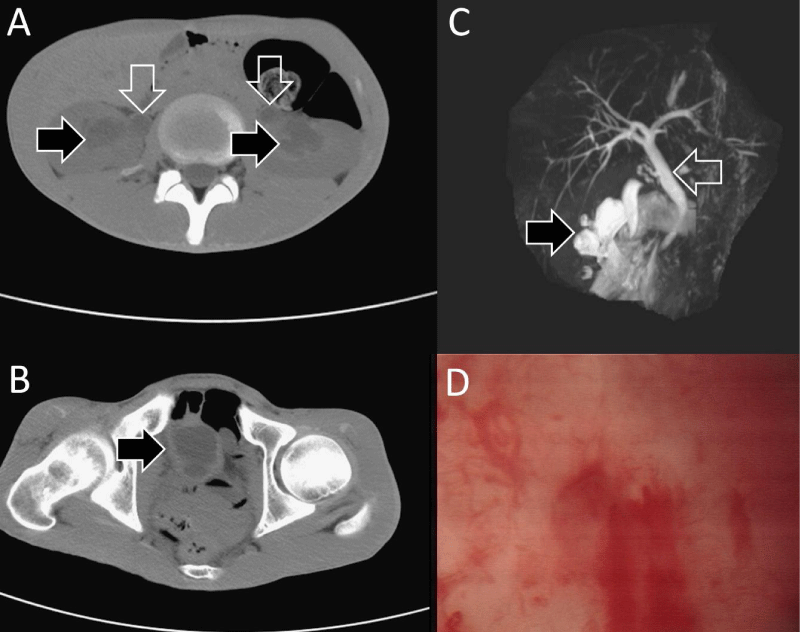
Figure 1: Bilateral hydronephrosis (black arrows in panel A), hydroureter (white arrows in panel A), irregular thickened wall of urinary bladder (black arrow in panel B), fusiform common bile duct with distal stenosis (panel C), and ulcerative cystitis (panel D).
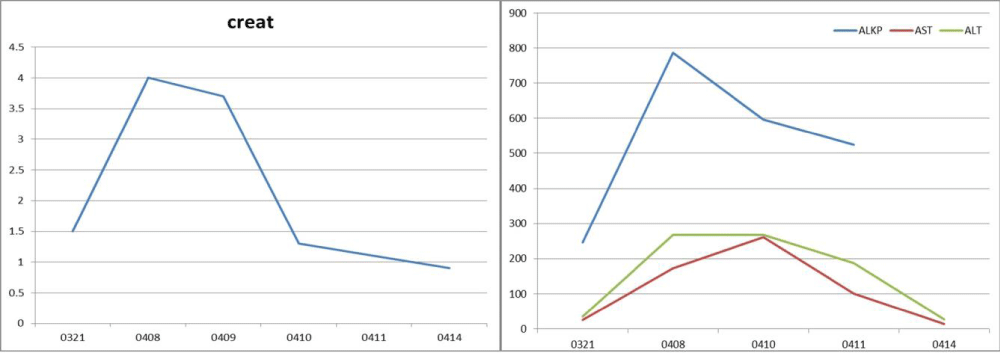
Figure 2: Creatinine (left panel), ALKP, AST, and ALT (right panel) returned to normal limits.
KAUC was first identified by lower urinary tract symptoms (LUTS) in 2007. Mechanisms of ketamine-related urological and gastrointestinal damages include direct toxic injury, microvascular damage, and autoimmunity triggered by ketamine and its metabolites. Clinicians should be aware of this clinical entity and able to recognize it when patients present unexplained gastrointestinal symptoms and LUTS [1,2].
This study was approved by the Institutional Review Board of Taichung Veterans General Hospital (No. CE19152A).
This work was supported by grants from the Taichung Veterans General Hospital (Grant numbers: TCVGH-109 7202C).
- Middela S, Pearce I. Ketamine-induced vesicopathy: a literature review. Int J Clin Pract. 2011; 65: 27-30. PubMed: https://pubmed.ncbi.nlm.nih.gov/21155941/
- Yu WL, Cho CC, Lung PF, Hung EHY, Hui JWY, et al. Ketamine-related cholangiopathy: a retrospective study on clinical and imaging findings. Abdom Imaging. 2014; 39: 1241-1246. PubMed: https://pubmed.ncbi.nlm.nih.gov/24934474/